The high prevalence of paediatric emergencies in rural and remote Australia necessitates that health professionals prioritise expertise in both paediatrics and emergency management.
In Fitzroy Crossing, WA, a study by Dossetor et al¹ revealed that a staggering 82% of children in the community visited the emergency department (ED) at least once, with 32% experiencing more than 11 presentations over a five-year period.
The challenges inherent in delivering emergency care to children in low-resource settings are often compounded by the presence of chronic conditions, complex needs, barriers to service delivery, poor infrastructure, and cross-cultural considerations.
Interventions in these settings must also be tailored to the specific emergency context and align with the policies of the employing health service.
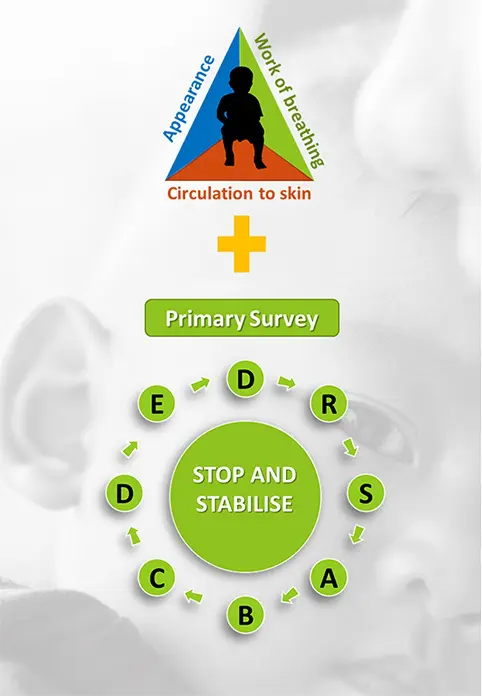
Paediatric Assessment Triangle (PAT)
The Paediatric Assessment Triangle (PAT)², used alongside the primary survey, provides
a structured approach to quickly identify potentially life-threatening conditions in children, ensuring timely and appropriate interventions.
It is a visual and hands-off tool that helps health workers assess a child’s condition within seconds.
PAT focuses on three critical components:
- Appearance: This includes the child’s tone, interactiveness, consolability, look/gaze, and speech/cry. A child who is alert, interactive, and has a normal cry or speech is generally stable. Conversely, a child who is lethargic, irritable, or has an abnormal cry may be in distress.
- Work of breathing: Observing the effort a child makes to breathe can reveal respiratory distress. Signs include nasal flaring, retractions, grunting, or abnormal breath sounds. Normal, effortless breathing indicates stability.
- Circulation to skin: This involves checking the child’s skin colour and temperature. Normal skin colour and warmth suggest good circulation, while pallor, mottling, or cyanosis can indicate poor perfusion and potential shock.
By combining the PAT with the primary survey, health professionals can rapidly and effectively assess paediatric patients.
This structured approach ensures that potentially life-threatening conditions are identified and managed promptly, improving outcomes for children in rural and remote settings.
What is your level of confidence in assessing and responding to ill or injured paediatric patients? If you have some gaps in your knowledge or could do with an update, a CRANAplus Paediatric Emergency Care & Paediatric Advanced Life Support (PEC+PALS) course could be for you!
References
- Dossetor PJ, Fitzpatrick EFM, Glass K, et al. Emergency department presentations by children in remote Australia: a population- based study. Glob. Pediatr. Health. 2021;8. doi:10.1177/2333794X21991006
- Horeczko T, Enriquez B, McGrath NE, Gausche-Hill M, Lewis RJ. The Pediatric Assessment Triangle: accuracy of its application by nurses in the triage of children. J. Emerg. Nurs. 2013; 39(2):182-189. doi: 10.1016/j.jen.2011.12.020